Cost-effective Legionella control starts with risk assessment.
Don’t shoot the messenger .... says Andrew Steel, Managing Director of Airmec
Don’t shoot the messenger .... says Andrew Steel, Managing Director of Airmec
This article was first published in Health Estate, March 2013
VIEW DIGITAL ISSUE online in the HEJ Archive - you may need to register (for free)
VIEW DIGITAL ISSUE online in the HEJ Archive - you may need to register (for free)
Managers of healthcare trusts may feel themselves to be caught between a rock and a hard place on any number of issues, and Legionella control was never going to be an exception. When prevention measures fail and a positive result is returned from the lab, there is an imperative to act fast to stamp infection out, but taking the right action is never going to be easy.
Fulfilling a healthcare provider’s duty of care to eradicate the infection, and do as much as possible to prevent repetition, will usually mean both major disruption and significant expenditure.
Shutting down operational areas of the building is a major logistical exercise and expensive in itself, before you even factor in the cost of disinfection, and remedial work.
Even though a Legionella positive result does not always mean that immediate shut down is essential, there is never going to be much time for delay; and institutional checks and balances make it difficult to authorise significant expenditure quickly enough. There may simply be no time for competitive tendering or normal due process. It’s the finance director’s nightmare – one that hav ing good risk assessment in place can help to avoid.
As a business with significant experience of working with healthcare trusts, air and water treatment specialists Airmec has first hand knowledge of working with Trusts who have been faced with the dreaded combination of Legionella-positive lab results, no budget for the remedial works necessary and no time for the due process that ought to be followed before commissioning works of such necessity. However, advising heath estates managers and financial chiefs of the consequences of infection can be a thankless task, says Airmec MD Andrew Steel.
“We’re not bringing good news, but please don’t shoot the messenger! Independent lab tests speak for themselves, and the seriousness of the predicament usually sinks in fairly quickly. After all, the law will hold responsible persons to account for failure to deal with the situation.”
While newer buildings may have the advantage of zoned water systems and built-in flushing valves, systems in older buildings are often a mystery even to the people who manage them. There will be a history of refurbishments and minor works such that no-one really knows the system, or could locate every pipe, outlet and potential risk area. Again, having a good, current and legally compliant risk assessment would mean that all this investigative trace-and-access work is in the bag.
If there is a Legionella positive result then getting rid of infection and avoiding a major incident in a sizeable health estate will typically involve several stages and potentially six figure sums. Thus may include:
Fulfilling a healthcare provider’s duty of care to eradicate the infection, and do as much as possible to prevent repetition, will usually mean both major disruption and significant expenditure.
Shutting down operational areas of the building is a major logistical exercise and expensive in itself, before you even factor in the cost of disinfection, and remedial work.
Even though a Legionella positive result does not always mean that immediate shut down is essential, there is never going to be much time for delay; and institutional checks and balances make it difficult to authorise significant expenditure quickly enough. There may simply be no time for competitive tendering or normal due process. It’s the finance director’s nightmare – one that hav ing good risk assessment in place can help to avoid.
As a business with significant experience of working with healthcare trusts, air and water treatment specialists Airmec has first hand knowledge of working with Trusts who have been faced with the dreaded combination of Legionella-positive lab results, no budget for the remedial works necessary and no time for the due process that ought to be followed before commissioning works of such necessity. However, advising heath estates managers and financial chiefs of the consequences of infection can be a thankless task, says Airmec MD Andrew Steel.
“We’re not bringing good news, but please don’t shoot the messenger! Independent lab tests speak for themselves, and the seriousness of the predicament usually sinks in fairly quickly. After all, the law will hold responsible persons to account for failure to deal with the situation.”
While newer buildings may have the advantage of zoned water systems and built-in flushing valves, systems in older buildings are often a mystery even to the people who manage them. There will be a history of refurbishments and minor works such that no-one really knows the system, or could locate every pipe, outlet and potential risk area. Again, having a good, current and legally compliant risk assessment would mean that all this investigative trace-and-access work is in the bag.
If there is a Legionella positive result then getting rid of infection and avoiding a major incident in a sizeable health estate will typically involve several stages and potentially six figure sums. Thus may include:
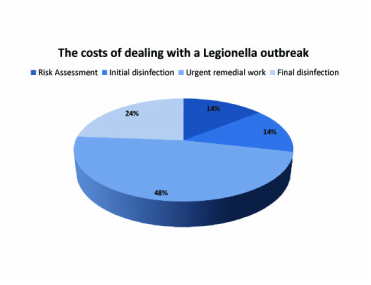
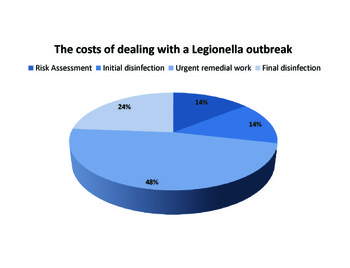
- Risk assessment to identify where the danger lies (dead legs, redundant piping etc).
- An initial disinfection to get the current outbreak under control (but will often not remove the root cause).
- Remedial work to remove major risks and likely causes of the current positive test results.
- Further disinfection and ongoing sampling, because remedial work such as the removal of system dead legs is very likely to disturb bacterial colonies and cause them to be distributed around the piping circuits.
The full risk assessment is highly significant here because in this recent example it should not have been necessary since it should already have been in place, enabling the water treatment professionals to confirm the cause of the infection and where it might have spread to more quickly and cost effectively.
Even where risk assessments are thought to be in place, their inadequacy can be quite staggering, according to Airmec. “By law, risk assessments should include schematic diagrams and be undertaken every two years, and more often if there have been changes to the system or indications that controls are failing.
All too frequently such risk assessments and accurate schematic diagrams are completely absent.” says Andrew Steel.
The chart shows how the costs were broken down in a recent £200,000 project.
The legal framework – and the extra burden for healthcare estates
The requirement for detailed schematics , and other, requirements for risk assessment are laid out quite clearly in the UK’s Health and Safety Executives (HSE) Approved Code of Practice and Guidance (ACOP) "Legionnaires' disease: Control of legionella bacteria in water systems" (L8) . L8 has special legal status and is legally binding: if designated responsible people within an organisation do not comply with its requirements the courts may hold them personally responsible for the consequences.
For healthcare estates, there is an additional requirement to adhere to the relevant Health Technical Memorandum (HTM). HTM 04-01 or to give it its full title “Health Technical Memorandum 04-01: The control of Legionella, hygiene, “safe” hot water, cold water and drinking water systems”. The current guidance was published by the Department of Health in 2006. HTM 04-01 builds on L8 but provides additional guidance to those involved with the control of Legionella in healthcare environments.
British Standard BS 8580:2010 Water quality – Risk assessments for Legionella control – Code of practice clearly lays out the best practice for risk assessments, but takes the form of guidance and recommendations rather than being a definitive specification. Since this document was first published in 2010 it is not referred to in the current edition of HTM 04-01, but prudent health estates managers would certainly wish to consider the recommendations contained within this document. Experienced water hygiene specialists will certainly be familiar with these recommendations, and undertake risk assessments that conform to the best practices laid out in this document. A key requirement of HTM04-01 is that risk assessments should be carried out by competent persons, so it is all the more surprising that good risk assessments are nowhere near ubiquitous.
A risk assessment identifies any reasonably foreseeable risks to health, and advises on the necessary precautionary measures that need to be taken to prevent, or adequately control, the risk. Of course, prevention is always going to be better – and more cost effective – than cure.
The risk assessment also enables the person on whom the statutory duty falls to show that all the steps needed to prevent or control foreseeable risk have been considered.
Risk assessments should be undertaken before the maintenance regime is put in place – or as soon as possible afterwards. This is especially important with so many trusts now preferring to manage routine work internally. It’s a logical approach that offers significant cost savings, says Airmec, but these will quickly be wiped out if the regime fails to address the risks and there is an outbreak. Professional help in aligning monitoring, inspection and flushing schedules with the asset register and schematic in the risk assessment is undoubtedly a good investment and one that will add further value to the risk assessment as a valuable tool for preventing outbreaks in the first place.
It’s also worth remembering that a risk assessment is a live document, not a one-off exercise. It is important that it is reviewed regularly and, ideally, in anticipation of rather than in response to changes.
Wise estates managers reading this article will be double checking their risk assessments as soon as possible – and be happy that they are not the ones juggling the need for urgent action with the budgetary constraints of the NHS….yet.
(HTM) 04-01 and HSE ACOP L8 – how do they work together?
L8, or to give it its full title - “Legionnaires’ disease -The control of legionella bacteria in water systems APPROVED CODE OF PRACTICE AND GUIDANCE” was first published in 2000. It was issued by the Health and Safety Commission (HSC) and Executive (HSE). As previously mentioned, it is very important to note that this code has been approved by the Health & Safety Commission SC with the consent of the Secretary of State, and has a special legal status, namely: “If you are prosecuted for breach of H&S law, and it is proved that you did not follow the relevant provisions of the Code, you will need to show that you have complied with the law in some other way or a Court will find you at fault”. In other words in these circumstances you are assumed to be guilty unless you can prove otherwise. The Department of Health published HTM 04 – 01: The control of Legionella, hygiene, “safe” hot water, cold water and drinking water systems in 2006. Health estates manager who comply with the operational processes outlined in this document will also meet the requirements of ACOP L8. In fact HTM 04-01 is actually more stringent in a number of areas.
L8, or to give it its full title - “Legionnaires’ disease -The control of legionella bacteria in water systems APPROVED CODE OF PRACTICE AND GUIDANCE” was first published in 2000. It was issued by the Health and Safety Commission (HSC) and Executive (HSE). As previously mentioned, it is very important to note that this code has been approved by the Health & Safety Commission SC with the consent of the Secretary of State, and has a special legal status, namely: “If you are prosecuted for breach of H&S law, and it is proved that you did not follow the relevant provisions of the Code, you will need to show that you have complied with the law in some other way or a Court will find you at fault”. In other words in these circumstances you are assumed to be guilty unless you can prove otherwise. The Department of Health published HTM 04 – 01: The control of Legionella, hygiene, “safe” hot water, cold water and drinking water systems in 2006. Health estates manager who comply with the operational processes outlined in this document will also meet the requirements of ACOP L8. In fact HTM 04-01 is actually more stringent in a number of areas.
One example of HTM04 – 01 exceeding the requirements of ACOP L8 is the treatment of water outlets that are not in regular use. ACOP L8 states that such outlets should be flushed weekly. HTM 04-01 suggests that such outlets should be flushed more frequently, and should form part of the daily cleaning process.
In practice it can be very difficult for managers to determine those outlets that are regularly used and those that are not (unless an area has been closed down). The only reliable way of doing this is to:
The other key area in terms of regular monitoring defined by both HTM 04-01 and ACOP L8 is the Temperature Control Regimen. HTM 04 - 01 details the tests to be carried out on hot and cold water outlets, and the standard frequency is monthly for all sentinel taps, typically the first and last taps on a hot water recirculating system or the nearest and furthest taps from the tank on a cold water system. . All results should be logged using a standard template, an example of which is also contained within the document.
Biological monitoring is not generally considered necessary unless there are taste or odour issues, however HTM04-01 does make it clear that the infection control team will need to consider the level of risk and decide if such monitoring should take place. Section 10.2 details the situations where biological monitoring may be required, one example of which is if water storage and distribution temperatures do not achieve the levels required by the temperature control regimen. If biological monitoring is required British Standard BS 7592:2008 Sampling for Legionella bacteria in water systems – Code of practice lays out recommendations and best practice for such monitoring. Since this standard was published after the current edition of HTM04-01 (published October 2006) health estates manager would be well advised to consider these recommendations if biological monitoring is necessary.
HTM 04-01 is very clear that there must be a nominated Responsible Person in the organisation, appointed in writing by the management, who possesses adequate professional knowledge and training to devise and manage the necessary procedures to ensure the quality of the water in healthcare premises is maintained. This person should be a manager or director with sufficient authority to ensure that all procedures in place are carried out in a timely and effective manner. Although the definition of a responsible person in HTM 04-01 is similar to that defined in ACOP L8, the HTM again goes further. Paragraph 6.5 of the HTM document suggests that a responsible person should ideally be a chartered engineer, microbiologist or other professionally qualified person.
So, in summary, a health estates Manager who puts in place and operates systems as defined in HTM 04-01 can also be confident that they are meeting the requirement of ACOP L8. In addition they will be managing a regime which provides best practice in terms of legionella control and water system management for the specific needs of health estates and their stakeholders.
Even where risk assessments are thought to be in place, their inadequacy can be quite staggering, according to Airmec. “By law, risk assessments should include schematic diagrams and be undertaken every two years, and more often if there have been changes to the system or indications that controls are failing.
All too frequently such risk assessments and accurate schematic diagrams are completely absent.” says Andrew Steel.
The chart shows how the costs were broken down in a recent £200,000 project.
The legal framework – and the extra burden for healthcare estates
The requirement for detailed schematics , and other, requirements for risk assessment are laid out quite clearly in the UK’s Health and Safety Executives (HSE) Approved Code of Practice and Guidance (ACOP) "Legionnaires' disease: Control of legionella bacteria in water systems" (L8) . L8 has special legal status and is legally binding: if designated responsible people within an organisation do not comply with its requirements the courts may hold them personally responsible for the consequences.
For healthcare estates, there is an additional requirement to adhere to the relevant Health Technical Memorandum (HTM). HTM 04-01 or to give it its full title “Health Technical Memorandum 04-01: The control of Legionella, hygiene, “safe” hot water, cold water and drinking water systems”. The current guidance was published by the Department of Health in 2006. HTM 04-01 builds on L8 but provides additional guidance to those involved with the control of Legionella in healthcare environments.
British Standard BS 8580:2010 Water quality – Risk assessments for Legionella control – Code of practice clearly lays out the best practice for risk assessments, but takes the form of guidance and recommendations rather than being a definitive specification. Since this document was first published in 2010 it is not referred to in the current edition of HTM 04-01, but prudent health estates managers would certainly wish to consider the recommendations contained within this document. Experienced water hygiene specialists will certainly be familiar with these recommendations, and undertake risk assessments that conform to the best practices laid out in this document. A key requirement of HTM04-01 is that risk assessments should be carried out by competent persons, so it is all the more surprising that good risk assessments are nowhere near ubiquitous.
A risk assessment identifies any reasonably foreseeable risks to health, and advises on the necessary precautionary measures that need to be taken to prevent, or adequately control, the risk. Of course, prevention is always going to be better – and more cost effective – than cure.
The risk assessment also enables the person on whom the statutory duty falls to show that all the steps needed to prevent or control foreseeable risk have been considered.
Risk assessments should be undertaken before the maintenance regime is put in place – or as soon as possible afterwards. This is especially important with so many trusts now preferring to manage routine work internally. It’s a logical approach that offers significant cost savings, says Airmec, but these will quickly be wiped out if the regime fails to address the risks and there is an outbreak. Professional help in aligning monitoring, inspection and flushing schedules with the asset register and schematic in the risk assessment is undoubtedly a good investment and one that will add further value to the risk assessment as a valuable tool for preventing outbreaks in the first place.
It’s also worth remembering that a risk assessment is a live document, not a one-off exercise. It is important that it is reviewed regularly and, ideally, in anticipation of rather than in response to changes.
Wise estates managers reading this article will be double checking their risk assessments as soon as possible – and be happy that they are not the ones juggling the need for urgent action with the budgetary constraints of the NHS….yet.
(HTM) 04-01 and HSE ACOP L8 – how do they work together?
L8, or to give it its full title - “Legionnaires’ disease -The control of legionella bacteria in water systems APPROVED CODE OF PRACTICE AND GUIDANCE” was first published in 2000. It was issued by the Health and Safety Commission (HSC) and Executive (HSE). As previously mentioned, it is very important to note that this code has been approved by the Health & Safety Commission SC with the consent of the Secretary of State, and has a special legal status, namely: “If you are prosecuted for breach of H&S law, and it is proved that you did not follow the relevant provisions of the Code, you will need to show that you have complied with the law in some other way or a Court will find you at fault”. In other words in these circumstances you are assumed to be guilty unless you can prove otherwise. The Department of Health published HTM 04 – 01: The control of Legionella, hygiene, “safe” hot water, cold water and drinking water systems in 2006. Health estates manager who comply with the operational processes outlined in this document will also meet the requirements of ACOP L8. In fact HTM 04-01 is actually more stringent in a number of areas.
L8, or to give it its full title - “Legionnaires’ disease -The control of legionella bacteria in water systems APPROVED CODE OF PRACTICE AND GUIDANCE” was first published in 2000. It was issued by the Health and Safety Commission (HSC) and Executive (HSE). As previously mentioned, it is very important to note that this code has been approved by the Health & Safety Commission SC with the consent of the Secretary of State, and has a special legal status, namely: “If you are prosecuted for breach of H&S law, and it is proved that you did not follow the relevant provisions of the Code, you will need to show that you have complied with the law in some other way or a Court will find you at fault”. In other words in these circumstances you are assumed to be guilty unless you can prove otherwise. The Department of Health published HTM 04 – 01: The control of Legionella, hygiene, “safe” hot water, cold water and drinking water systems in 2006. Health estates manager who comply with the operational processes outlined in this document will also meet the requirements of ACOP L8. In fact HTM 04-01 is actually more stringent in a number of areas.
One example of HTM04 – 01 exceeding the requirements of ACOP L8 is the treatment of water outlets that are not in regular use. ACOP L8 states that such outlets should be flushed weekly. HTM 04-01 suggests that such outlets should be flushed more frequently, and should form part of the daily cleaning process.
In practice it can be very difficult for managers to determine those outlets that are regularly used and those that are not (unless an area has been closed down). The only reliable way of doing this is to:
- produce an asset register identifying location of all outlets
- develop a clear maintenance plan with agreed responsibilities for staff undertaking the flushing regime
- compile a log book to record flushing activities
- ensure that training, spot checks and supervision are then implemented to ensure that staff realise the significance of their work and ensure that the tests are carried out
The other key area in terms of regular monitoring defined by both HTM 04-01 and ACOP L8 is the Temperature Control Regimen. HTM 04 - 01 details the tests to be carried out on hot and cold water outlets, and the standard frequency is monthly for all sentinel taps, typically the first and last taps on a hot water recirculating system or the nearest and furthest taps from the tank on a cold water system. . All results should be logged using a standard template, an example of which is also contained within the document.
Biological monitoring is not generally considered necessary unless there are taste or odour issues, however HTM04-01 does make it clear that the infection control team will need to consider the level of risk and decide if such monitoring should take place. Section 10.2 details the situations where biological monitoring may be required, one example of which is if water storage and distribution temperatures do not achieve the levels required by the temperature control regimen. If biological monitoring is required British Standard BS 7592:2008 Sampling for Legionella bacteria in water systems – Code of practice lays out recommendations and best practice for such monitoring. Since this standard was published after the current edition of HTM04-01 (published October 2006) health estates manager would be well advised to consider these recommendations if biological monitoring is necessary.
HTM 04-01 is very clear that there must be a nominated Responsible Person in the organisation, appointed in writing by the management, who possesses adequate professional knowledge and training to devise and manage the necessary procedures to ensure the quality of the water in healthcare premises is maintained. This person should be a manager or director with sufficient authority to ensure that all procedures in place are carried out in a timely and effective manner. Although the definition of a responsible person in HTM 04-01 is similar to that defined in ACOP L8, the HTM again goes further. Paragraph 6.5 of the HTM document suggests that a responsible person should ideally be a chartered engineer, microbiologist or other professionally qualified person.
So, in summary, a health estates Manager who puts in place and operates systems as defined in HTM 04-01 can also be confident that they are meeting the requirement of ACOP L8. In addition they will be managing a regime which provides best practice in terms of legionella control and water system management for the specific needs of health estates and their stakeholders.